At The Brain and Spine Centre, we specialize in the diagnosis and surgical treatment of neurological and spinal disorders. Dr. Muhammad Aqeel Natt, a leading neurosurgeon in Lahore, provides advanced, safe, and compassionate care for patients.
Craniosynostosis
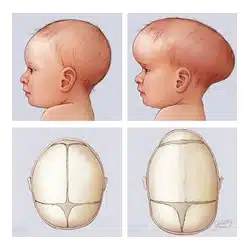
Craniosynostosis is a birth condition in which one or more of a baby’s skull sutures (the flexible joints between skull bones) fuse too early, before the brain has finished growing. This premature fusion restricts skull growth in the closed suture and forces growth in remaining open sutures, leading to an abnormally shaped head and, in some cases, raised pressure inside the skull.
Our goal is simple: diagnose early, reshape and expand the skull safely, and give the growing brain enough room to develop normally.
What Is Craniosynostosis?
In a typical infant, skull bones are separated by sutures that stay open to allow the skull to expand as the brain grows. In craniosynostosis, one or more sutures close prematurely, resulting in:
- Abnormal head shape based on which suture is fused (e.g., long narrow head in sagittal synostosis, short wide head in bicoronal synostosis)
- Compensatory overgrowth in regions where sutures remain open
- Possible restriction of intracranial volume if multiple sutures are affected, increasing the risk of raised intracranial pressure
- Types include:
- Nonsyndromic craniosynostosis: isolated suture fusion, usually with no identifiable cause
- Syndromic craniosynostosis: associated with genetic syndromes such as Apert, Crouzon, and Pfeiffer
Symptoms of Craniosynostosis
The most obvious early sign is an abnormally shaped head.
Common features:
• Abnormal skull shape (plagiocephaly, scaphocephaly, brachycephaly) depending on the fused suture
• Ridging over a fused suture (raised, hard ridge along the skull)
• Facial asymmetry such as one eye positioned higher, forehead flattening on one side, or a rotated nose in unicoronal synostosis
• Abnormal position or early closure of the soft spot (fontanel)
Signs of raised intracranial pressure (more common in multisuture or syndromic cases):
• Headache, nausea, vomiting, lethargy
• “Setting sun” eye sign or bulging, tense fontanel
• Developmental delay, visual problems, seizures, or learning difficulties if untreated
Diagnosis
Diagnosis combines clinical examination and imaging.
Physical exam assesses head shape, suture ridging, fontanel status, facial asymmetry, and head circumference growth curves.
Imaging:
• Skull X-ray or ultrasound can suggest fused sutures in infants.
• CT with 3D reconstruction is the standard for confirming which sutures are fused and the degree of deformity.
• MRI may be used when concerned about associated brain malformations or raised intracranial pressure.
Genetic evaluation is considered when syndromic craniosynostosis is suspected (e.g., associated limb anomalies, midface hypoplasia, airway issues).
Treatment Options
Early treatment, ideally within the first year of life, provides the best chance to normalize skull shape and prevent raised intracranial pressure.
Non-surgical options:
Positional molding (helmet therapy) can help with positional plagiocephaly but does not correct true craniosynostosis because fused sutures cannot expand.
Surgical options:
Goals: release fused sutures, reshape the skull, and increase intracranial volume.
Minimally invasive endoscopic suturectomy is usually performed in very young infants (often before 4–6 months) followed by postoperative helmet therapy.
Open cranial vault remodeling is used for older infants or more complex deformities, allowing comprehensive reshaping of the skull and orbits.
Choice of procedure depends on age, sutures involved, severity, presence of syndromic features, and intracranial pressure status.
The Procedure
Our management pathway focuses on safe, timely correction and long-term follow-up.
Multidisciplinary assessment including neurosurgery, craniofacial surgery, pediatrics, ophthalmology (for visual issues), and genetics for syndromic cases.
Surgical planning based on CT 3D reconstruction to determine incision, bone cuts, and reshaping strategy.
Under general anesthesia, the fused sutures are released; bone segments are reshaped and repositioned to normalize skull shape and increase volume, with resorbable plates/sutures as needed.
For endoscopic techniques, small incisions and targeted suture removal are followed by helmet therapy to guide skull growth.
Recovery & Aftercare
Recovery is usually well tolerated with specialized perioperative care.
Hospital stay typically ranges from 2–5 days depending on procedure type and complexity.
Swelling and bruising around the eyes are common in the first week and gradually resolve.
Follow-up includes head circumference monitoring, neurodevelopmental assessments, ophthalmologic checks, and periodic imaging when indicated.
Long-term outlook is generally good; most children treated early achieve normal or near-normal head shape and typical cognitive development.
Results You Can Expect
With timely and appropriate surgery:
Skull shape is significantly improved, often approaching typical appearance.
Risk of raised intracranial pressure and its complications (visual loss, cognitive impairment, seizures) is significantly reduced.
Most nonsyndromic craniosynostosis patients have normal intelligence and no major neurological deficits when treated early.
Syndromic craniosynostosis may require additional procedures (midface advancement, airway surgery) and closer neurodevelopmental surveillance.
Why Choose The Brain and Spine Centre
Led by Dr. Muhammad Aqeel Natt, with expertise in pediatric neurosurgery and craniofacial skull remodeling. Comprehensive evaluation using modern CT/MRI-based planning and multidisciplinary cooperation with craniofacial, pediatric, and ophthalmology teams. Tailored surgical approach (endoscopic vs. open remodeling) based on age, suture involvement, and severity, with emphasis on safety, esthetic outcome, and brain protection. Long-term follow-up to monitor growth, development, and need for any additional interventions.
Cost of Craniosynostosis Treatment
Costs vary with imaging, type of surgery (endoscopic vs. open), hospital stay, need for helmet therapy, and long-term follow-up and rehabilitation. Personalized estimates are provided after full clinical and imaging assessment.
Frequently Asked Questions (FAQs)
Can I know Dr. Muhammad Aqeel Natt’s credentials?
What types of brain tumours do you treat?
Is the surgery safe?
Do I need long-term follow-up after surgery?
Are you having health problems? Contact us today!
Address Business
Contact With Us
Call Us 24/7: 0318 4065914
Working Time
Sunday: 8.30am - 19.30pm