At The Brain and Spine Centre, we specialize in the diagnosis and surgical treatment of neurological and spinal disorders. Dr. Muhammad Aqeel Natt, a leading neurosurgeon in Lahore, provides advanced, safe, and compassionate care for patients.
Nerve Repair Surgery
Nerve repair surgery restores continuity and function of injured peripheral nerves using microsurgical techniques, nerve grafts, or nerve transfers when spontaneous recovery is unlikely. At The Brain and Spine Centre, Dr. Muhammad Aqeel Natt offers specialised nerve repair and reconstruction at Farooq Hospital, West Wood Branch, Lahore, focusing on precise microsurgery and early intervention to maximise recovery.
Our goal is simple: reconnect or reroute damaged nerves in time for meaningful reinnervation, relieve neuropathic pain, and recover as much strength and sensation as possible.
What Is Nerve Repair Surgery?
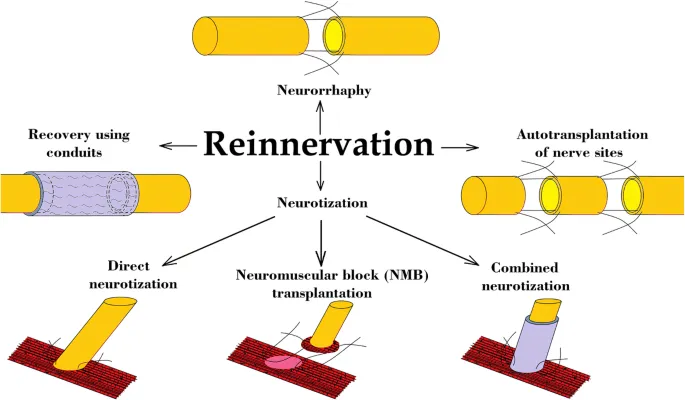
Peripheral nerve repair surgery encompasses a spectrum of techniques:
Direct end‑to‑end repair (neurorrhaphy): the preferred method when nerve ends can be approximated tension‑free; coaptation can be epineurial, fascicular, or group fascicular.
Epineural sleeve reconstruction: using redundant epineurium to bridge small gaps (up to ~10–14 mm) and cover the coaptation site, improving alignment, repair strength, and potentially accelerating regeneration.
Nerve grafting (autograft/allograft): interpositional grafts bridge segmental defects where direct repair would be under tension; sural nerve is most commonly used, and vascularised grafts are considered in scarred beds.
Nerve transfers (neurotisation): rerouting a functioning but less critical donor nerve (or fascicle) to reinnervate a more important denervated nerve closer to the target muscle, reducing regeneration distance and improving specificity.
Choice of technique depends on level and type of injury (sharp vs crush vs avulsion), gap length, time since injury, and functional priorities.
Symptoms and Indications
Nerve repair is considered when there is structural nerve disruption or when recovery is inadequate with conservative care.
Typical indications:
Sharp lacerations with complete or high‑grade nerve transection.
Segmental nerve loss after open trauma requiring grafting or nerve transfer.
Iatrogenic nerve injuries after surgery.
Failure of spontaneous recovery in closed injuries by 3–6 months (depending on nerve and level).
Painful neuromas requiring excision and reconstruction.
Motor nerves and mixed nerves are time‑critical because denervated muscles lose reinnervation potential over time; sensory‑only nerves tolerate longer delays but still benefit from earlier repair.
Diagnosis
Accurate diagnosis and planning rely on:
Clinical examination mapping motor deficits, sensory loss, Tinel’s progression, and functional impairment.
Electrodiagnostic testing (EMG/NCS) to assess denervation, reinnervation, and distinguish neuropraxia from axonotmesis/neurotmesis.
High‑resolution ultrasound and MRI neurography to visualise nerve continuity, neuromas, and entrapment.
The Procedure
Nerve repair surgery is performed under magnification using microsurgical instruments.
Key steps:
Exploration and debridement: unhealthy nerve ends and scar tissue are excised back to healthy fascicles.
Direct repair:
End‑to‑end neurorrhaphy using 8‑0–10‑0 nylon with careful alignment of fascicular groups and epineurial landmarks, avoiding tension.
Epineural repair is common; fascicular or group fascicular repair may be chosen in large polyfascicular nerves where fascicle groups can be matched.
Epineural sleeve: epineurium from one stump is advanced over the coaptation to bridge small gaps and protect the repair site.
Nerve grafting:
For longer gaps, autologous nerve (e.g., sural nerve) is harvested and interposed; vascularised grafts are used when the bed is scarred or poorly vascularised.
Nerve transfers:
Donor fascicles or nerves (e.g., redundant motor branches) are coapted closer to target muscles to shorten regeneration distance; typically only one neurorrhaphy site is created, improving outcomes vs long grafts.
Timing:
Clean sharp injuries: primary repair ideally within 72 hours–14 days yields best outcomes.
Mixed motor nerves: optimal primary repair within 3 days; purely sensory nerves preferably within 7–14 days, but up to 3 months remains reasonable for sensory recovery.
Delayed presentations: reconstruct within 3–6 months to avoid irreversible motor end‑plate loss; after that, nerve transfers and muscle transfers are often needed.
Recovery & Aftercare
Nerve regeneration proceeds at roughly 1–3 mm/day from the repair site; functional recovery may take 6–24 months depending on distance to target.
Regular follow‑up with EMG and clinical exams tracks reinnervation and guides therapy.
Physiotherapy and occupational therapy are crucial to maintain joint mobility, prevent contractures, strengthen reinnervated muscles, and retrain sensory function.
Pain management addresses neuropathic pain and neuroma‑related discomfort.
Results You Can Expect
Outcomes depend on nerve, level, patient age, timing, and technique.
Early repairs (within 2 weeks) of clean sharp injuries show significantly higher rates of good–excellent functional results than delayed repairs; for example, nearly half of mixed nerves repaired within 14 days achieved good–excellent outcomes vs about one‑quarter in late repairs in one series.
Sensory nerves can regain useful function even when repaired later, though best results are with repairs within 3 months.
Nerve transfers often outperform long grafts in high‑level injuries because they reduce regeneration distance and improve axon specificity, especially for shoulder and elbow function.
Why Choose The Brain and Spine Centre
Led by Dr. Muhammad Aqeel Natt, with focused expertise in peripheral nerve microsurgery, nerve grafting, nerve transfers, and complex reconstructions after trauma or tumour surgery. Evidence‑based timing and technique selection guided by contemporary literature on nerve repair outcomes and regeneration windows. Use of high‑magnification microsurgery and modern techniques such as epineural sleeve neurorrhaphy, interposition grafting, and targeted nerve transfers to optimise functional recovery. Close integration with EMG services, physiotherapy, and pain management for comprehensive peri‑operative care.
Cost of Nerve Repair Surgery
Costs vary with injury complexity, number of nerves involved, need for grafts or transfers, operative time, hospital stay, and length of rehabilitation. Personalised estimates are provided after full assessment and imaging/electrodiagnostic review.
Frequently Asked Questions (FAQs)
Can I know Dr. Muhammad Aqeel Natt’s credentials?
What types of brain tumours do you treat?
Is the surgery safe?
Do I need long-term follow-up after surgery?
Are you having health problems? Contact us today!
Address Business
Contact With Us
Call Us 24/7: 0318 4065914
Working Time
Sunday: 8.30am - 19.30pm