At The Brain and Spine Centre, we specialize in the diagnosis and surgical treatment of neurological and spinal disorders. Dr. Muhammad Aqeel Natt, a leading neurosurgeon in Lahore, provides advanced, safe, and compassionate care for patients.
Hemorrhagic Stroke
Hemorrhagic stroke is a life-threatening emergency that needs rapid, expert care to control bleeding, relieve pressure on the brain, and prevent permanent disability or death. At The Brain and Spine Centre, Dr. Muhammad Aqeel Natt provides specialized hemorrhagic stroke care at Farooq Hospital, West Wood Branch, Lahore, integrating neurosurgical expertise with intensive stroke management.
Our goal is simple: stop or reduce bleeding, protect brain tissue, and support recovery for the best possible quality of life.
What Is a Hemorrhagic Stroke?
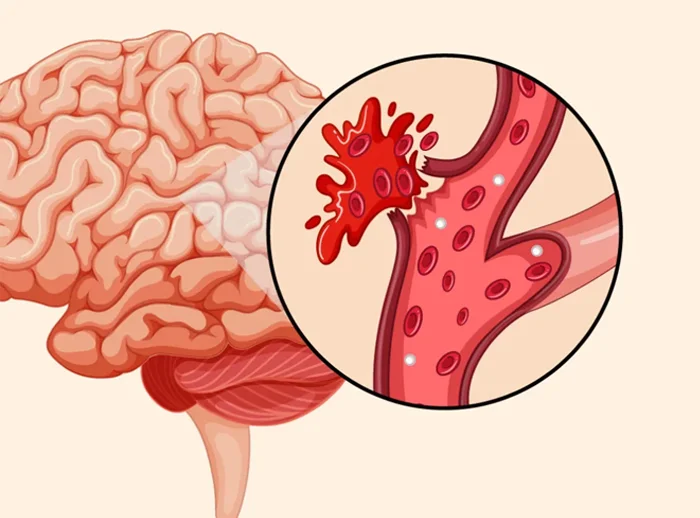
A hemorrhagic stroke happens when a blood vessel in or on the surface of the brain leaks or bursts, causing bleeding into the surrounding brain tissue or spaces around the brain. The bleeding leads to swelling, increased pressure inside the skull, and damage to brain cells in the affected area. Hemorrhagic stroke accounts for about 10–20% of all strokes and is generally more severe, with higher early mortality than ischemic stroke.
There are two main types:
- Intracerebral hemorrhage (ICH): Bleeding directly into the brain tissue, often from small arteries damaged by long-standing high blood pressure or cerebral amyloid angiopathy.
- Subarachnoid hemorrhage (SAH): Bleeding into the space around the brain, most commonly from a ruptured aneurysm or arteriovenous malformation (AVM).
Symptoms of Hemorrhagic Stroke
Symptoms typically start suddenly and require emergency evaluation.
Common warning signs include:
- Sudden severe headache, often described as the “worst headache of life,” especially in aneurysmal SAH
- Sudden weakness or paralysis of face, arm, or leg, usually on one side of the body
- Sudden difficulty speaking, understanding speech, or confusion
- Sudden vision problems such as double vision or loss of vision
- Sudden loss of balance, dizziness, trouble walking, or coordination problems
- Nausea, vomiting, decreased level of consciousness, or loss of consciousness
Any sudden stroke-like symptoms must be treated as an emergency. Do not wait for symptoms to improve.
Causes and Risk Factors
Common causes include:
- Long-standing high blood pressure (hypertension) damaging small brain arteries, the leading cause of spontaneous ICH
- Ruptured intracranial aneurysm causing subarachnoid hemorrhage
- Arteriovenous malformations (AVMs) and other vascular malformations
- Cerebral amyloid angiopathy (CAA), especially in older adults, causing lobar hemorrhages and microbleeds
- Head trauma
- Overtreatment with blood thinners (anticoagulants) and antiplatelet drugs
- Less commonly, tumors, vasculitis, or bleeding disorders
Major risk factors include uncontrolled hypertension, smoking, heavy alcohol use, older age, and previous stroke or hemorrhage.
Diagnosis
Rapid imaging is essential to distinguish hemorrhagic from ischemic stroke and guide treatment.
Key steps:
- Neurological examination to assess stroke severity and consciousness
- Non-contrast CT head is the gold-standard first test, rapidly detecting acute bleeding, its location, and size
- MRI with specialized sequences (GRE/SWI) can detect acute and chronic hemorrhage and associated lesions, but CT is faster and more widely available in emergencies
- CT or MR angiography identifies aneurysms, AVMs, or other vascular lesions requiring neurosurgical or endovascular treatment
- Laboratory tests, blood pressure evaluation, and coagulation studies guide acute management and correction of coagulopathy
Treatment Options
Management focuses on stabilizing the patient, controlling bleeding and pressure, and treating the underlying cause.
Key components:
- Blood pressure control: Gradual reduction of systolic blood pressure to approximately 140–160 mmHg in the first 24–48 hours is recommended in most patients to reduce risk of ongoing bleeding while maintaining adequate brain perfusion. Intravenous agents such as labetalol, nicardipine, or other antihypertensives are commonly used.
- Reversal of anticoagulation: Urgent reversal of blood thinners (e.g., vitamin K antagonists, DOACs, heparin) to limit hematoma expansion.
- Intracranial pressure (ICP) management: Head elevation, careful fluid management, and osmotic therapy as needed in neurocritical care settings.
Surgical options in selected cases:
- Surgical evacuation of hematoma may benefit patients with large cerebellar hemorrhages (>3 cm) causing brainstem compression or hydrocephalus, and some lobar hemorrhages with mass effect or neurological deterioration.
- Decompressive craniectomy with hematoma evacuation for large hypertensive hemispheric ICH in patients with low GCS scores can reduce mortality and improve outcomes in carefully selected patients.
- Aneurysm clipping or endovascular coiling to secure ruptured aneurysms in SAH.
- Resection or endovascular treatment of AVMs and other vascular malformations when appropriate.
All patients benefit from specialized stroke unit or neurocritical care with multidisciplinary management.
The Procedure (Acute Care Pathway)
Our process emphasizes speed, safety, and targeted intervention:
- Emergency assessment and CT head immediately on arrival to confirm hemorrhage and determine its type and location.
- Rapid blood pressure control, reversal of anticoagulation, and stabilization of airway, breathing, and circulation.
- Neurosurgical evaluation to determine need and timing for surgical evacuation, decompressive surgery, or aneurysm/AVM treatment.
- Transfer to stroke unit or ICU for close neurological and hemodynamic monitoring, management of complications such as hydrocephalus, seizures, or rebleeding, and initiation of early rehabilitation.
Recovery & Aftercare
Recovery after hemorrhagic stroke can be prolonged and often more challenging than after ischemic stroke, but many patients improve significantly with intensive care and rehabilitation.
- Early rehabilitation with physiotherapy, occupational therapy, and speech and swallowing therapy is crucial to regain mobility, independence, and communication.
- Blood pressure control is the key strategy to prevent recurrent hemorrhage and also lowers risk of future ischemic stroke and heart disease. Long-term antihypertensive therapy aiming at guideline BP targets provides up to 50% relative risk reduction in recurrent ICH for each 10 mmHg systolic reduction.
- Lifestyle changes including smoking cessation, moderating alcohol, healthy diet, exercise, and careful medication adherence are essential.
- Regular follow-up with neurology and primary care monitors neurologic recovery, BP control, and complications such as cognitive impairment or depression.
Results You Can Expect
Outcomes depend on hemorrhage size, location, level of consciousness on admission, age, and speed of treatment. Many patients experience substantial improvement over weeks to months with multidisciplinary care and strict blood pressure control. Long-term BP management substantially reduces risk of recurrent ICH and improves overall cardiovascular outcomes. Specialized stroke units are associated with better survival and reduced disability at one year for hemorrhagic stroke patients.
Why Choose The Brain and Spine Centre
Led by Dr. Muhammad Aqeel Natt, expert in neurosurgery and neurovascular care, with experience in managing intracerebral and subarachnoid hemorrhage requiring surgical and intensive care. Access to emergency CT and MRI, vascular imaging, and neurosurgical operating facilities for rapid diagnosis and intervention. Integration with ICU, stroke unit, and rehabilitation services to cover the full continuum from emergency treatment to long-term recovery. Convenient location at Farooq Hospital, West Wood Branch, Lahore for timely access in emergencies.
Cost of Hemorrhagic Stroke Treatment
Costs vary with hemorrhage size and location, need for ICU care, surgical or endovascular procedures, imaging frequency, and length and intensity of rehabilitation. Personalized estimates are provided after clinical evaluation and imaging review.
Frequently Asked Questions (FAQs)
Can I know Dr. Muhammad Aqeel Natt’s credentials?
What types of brain tumours do you treat?
Is the surgery safe?
Do I need long-term follow-up after surgery?
Are you having health problems? Contact us today!
Address Business
Contact With Us
Call Us 24/7: 0318 4065914
Working Time
Sunday: 8.30am - 19.30pm