At The Brain and Spine Centre, we specialize in the diagnosis and surgical treatment of neurological and spinal disorders. Dr. Muhammad Aqeel Natt, a leading neurosurgeon in Lahore, provides advanced, safe, and compassionate care for patients.
Spinal Stenosis
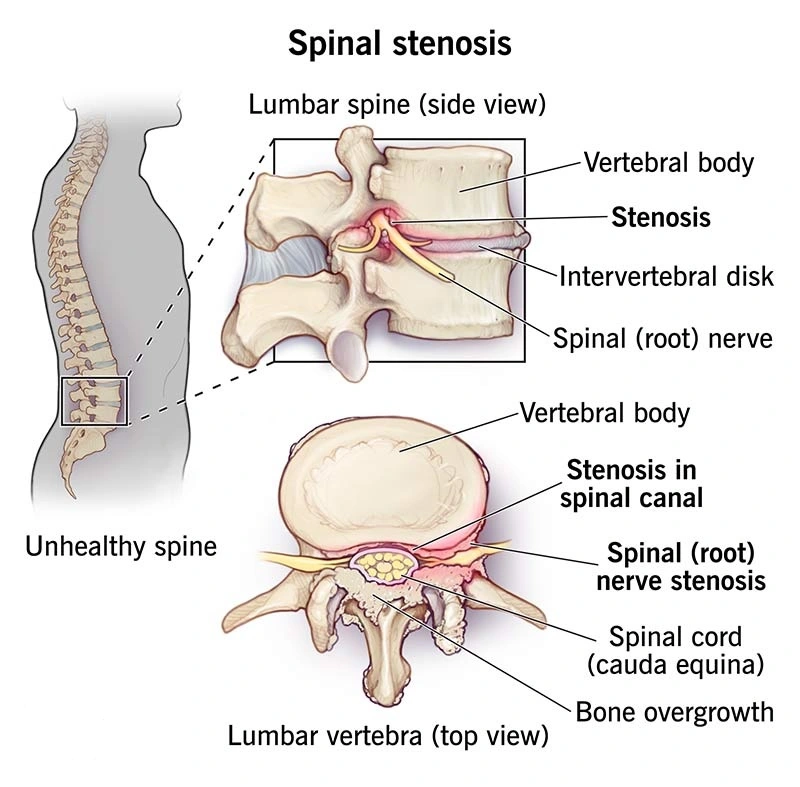
Spinal stenosis is a narrowing of the spinal canal that compresses the spinal cord or nerve roots, most commonly in the lumbar or cervical spine, causing pain, numbness, weakness, and reduced mobility. At The Brain and Spine Centre, Dr. Muhammad Aqeel Natt offers comprehensive management of spinal stenosis at Farooq Hospital, West Wood Branch, Lahore, from conservative therapies to minimally invasive decompression and fusion when indicated.
Our goal is simple: relieve nerve compression, reduce pain, and restore functional mobility while preserving spinal stability.
What Is Spinal Stenosis?
Spinal stenosis occurs when the spinal canal or neural foramina narrow, compressing neural elements; it is typically degenerative in adults over 50 but can be congenital or acquired. Lumbar stenosis (most common) affects the lower back and legs; cervical stenosis impacts the neck, arms, and sometimes cord function with greater risk of myelopathy.
Key causes:
Degenerative changes: disc bulging, ligamentum flavum thickening, facet hypertrophy, osteophytes.
Spondylolisthesis, prior surgery (iatrogenic), trauma, or congenital narrowing.
Symptoms of Spinal Stenosis
Symptoms develop gradually and classically worsen with extension (standing/walking) and improve with flexion (sitting/leaning forward).
Common features:
Low back pain, neurogenic claudication (leg pain/cramping/numbness/heaviness with walking, relieved by sitting).
Leg weakness, foot drop, balance issues.
Cervical: neck pain, arm radiculopathy, hand clumsiness, gait disturbance; severe cases cause myelopathy (spasticity, hyperreflexia, bowel/bladder dysfunction).
Red flags: progressive weakness, incontinence, falls indicate urgent intervention.
Diagnosis
Diagnosis combines clinical evaluation and imaging.
History and exam: neurogenic claudication pattern, straight-leg raise negative, extension worsens symptoms.
MRI: gold standard showing canal/foraminal narrowing (<10 mm AP diameter severe), cord/nerve compression, facet arthropathy.
X-ray/CT: bony anatomy, alignment, dynamic instability.
EMG/nerve conduction: confirms radiculopathy if needed.
Treatment Options
Most patients (~80-90%) improve with non-surgical care; surgery reserved for failure or red flags.
Conservative management:
NSAIDs, gabapentinoids, short-term opioids for pain.
Physical therapy: flexion-based exercises, core strengthening, cycling.
Epidural steroid injections: temporary relief (3-6 months).
Surgical indications:
Refractory symptoms >6-12 months, progressive neurology, instability, cauda equina.
Procedures:
Decompression: laminectomy, foraminotomy, microdiscectomy.
Fusion if instability/spondylolisthesis: percutaneous or open instrumentation.
The Procedure
At The Brain and Spine Centre:
Minimally invasive decompression: small incisions, tubular retractors, preserve paraspinals/ligamentum.
Laminectomy removes hypertrophic ligament/bone; foraminotomy enlarges exits; discectomy if herniation.
Fusion (if needed): percutaneous pedicle screws/rods +/- interbody cage.
Intraoperative neuromonitoring, fluoroscopy.
Recovery & Aftercare
Hospital: 1-3 days; walk day-of surgery.
PT starts immediately: gait training, flexion exercises.
Brace 4-6 weeks if fused; full recovery 3-6 months.
70-80% report major improvement; durable if no instability.
Results You Can Expect
Conservative: 50-70% satisfactory long-term.
Surgery: 70-90% leg pain relief; walking distance improves 3-5x; 10-20% reoperation (adjacent segment).
Risks: infection (1-2%), CSF leak, worsening deficit (<5%).
Why Choose The Brain and Spine Centre
Expertise in minimally invasive techniques reducing morbidity/recovery time. Advanced imaging/navigation for precise decompression. Multidisciplinary: pain management, PT, rehab for optimal outcomes.
Cost of Spinal Tumour Excision
Varies by conservative vs surgical; decompression ~lower cost than fusion. Estimates post-assessment.
Frequently Asked Questions (FAQs)
Can I know Dr. Muhammad Aqeel Natt’s credentials?
What types of brain tumours do you treat?
Is the surgery safe?
Do I need long-term follow-up after surgery?
Are you having health problems? Contact us today!
Address Business
Contact With Us
Call Us 24/7: 0318 4065914
Working Time
Sunday: 8.30am - 19.30pm