At The Brain and Spine Centre, we specialize in the diagnosis and surgical treatment of neurological and spinal disorders. Dr. Muhammad Aqeel Natt, a leading neurosurgeon in Lahore, provides advanced, safe, and compassionate care for patients.
Torticollis
Torticollis is a sustained involuntary contraction of neck muscles causing abnormal head posture, most commonly a twisting or tilting of the head to one side, resulting from cervical dystonia (idiopathic or acquired) and requiring multidisciplinary evaluation and management including botulinum toxin, physical therapy, and rarely surgery. At The Brain and Spine Centre, Dr. Muhammad Aqeel Natt manages torticollis at Farooq Hospital, West Wood Branch, Lahore, offering medical optimization, botulinum toxin injection, and surgical intervention for severe or refractory cases.
Our goal is simple: identify the underlying cause, relieve involuntary muscle spasm, restore normal head posture and cervical function, and improve quality of life.
What Is Torticollis?
Torticollis (wry neck) is an involuntary sustained contraction of cervical muscles—most commonly the sternocleidomastoid, trapezius, or splenius capitis—causing abnormal head posture (tilting, rotation, flexion, or extension). It may be congenital (fibrotic muscle shortening, bony abnormality) or acquired, with idiopathic cervical dystonia being the most common adult form.
Pathophysiology:
Idiopathic cervical dystonia: abnormal basal ganglia motor control causing involuntary co-contraction of agonist-antagonist muscles.
Secondary torticollis: spasticity from stroke, cerebral palsy, head trauma, Parkinson’s disease, medication side effects (antipsychotics), or structural spinal pathology.
Symptoms of Torticollis
Symptoms vary by type and severity.
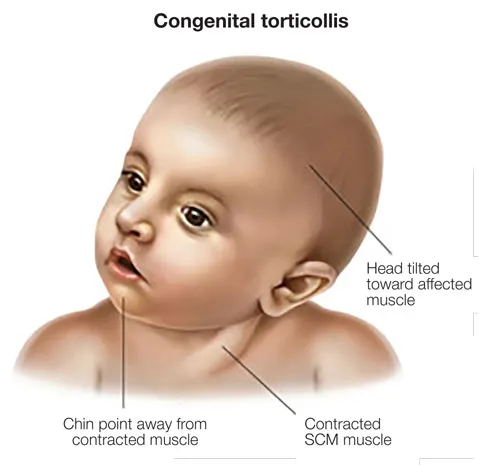
Congenital torticollis:
Head tilt noticed in infancy; sternocleidomastoid shortening palpable; associated asymmetric face if untreated.
Idiopathic cervical dystonia (adult-onset):
Involuntary neck muscle contraction, progressive over months-years.
Head posture deformity: rotatory (most common ~40%), laterocollis (tilting ~20%), antecollis (forward flexion), retrocollis (extension), or combination.
Associated tremor, pain (50-75% experience neck/shoulder pain from sustained contraction).
Sensory trick: many patients find specific touch or maneuver temporarily relieves symptoms (e.g., touching chin or cheek).
Psychosocial distress, social embarrassment, functional impairment (difficulty driving, reading, eating).
Secondary torticollis:
Spasticity features, hyperreflexia, associated weakness if neurological cause.
Pain, stiffness worse in morning after prolonged postures.
Diagnosis
Diagnosis is primarily clinical; imaging rules out structural causes.
Clinical evaluation: head posture documentation, active/passive range of motion, pain assessment, patient-reported disability (Toronto Western Spasmodic Torticollis Rating Scale—TWSTRS).
Imaging (if secondary suspected): cervical spine MRI to exclude syrinx, Chiari malformation, tethering, or other structural lesions; brain MRI for signs of basal ganglia pathology if onset in childhood/adolescence.
Electromyography (EMG): may show co-contraction pattern supporting diagnosis; not required for idiopathic cases.
Ancillary testing: exclude metabolic causes (Wilson disease with Kayser-Fleischer rings, hyperthyroidism) in young-onset or progressive cases.
Treatment Options
Conservative management:
Physical therapy: stretching, postural correction, muscle relaxation techniques; limited benefit alone but supportive.
Oral medications: baclofen, benzodiazepines (diazepam), anticholinergics (trihexyphenidyl); modest efficacy, limited by side effects.
Botulinum toxin (BoNT):
First-line treatment for idiopathic cervical dystonia; inhibits acetylcholine release, paralyzing overactive muscles.
Injected into hypertrophied/contracted muscles (sternocleidomastoid, trapezius, splenius capitis) under EMG or ultrasound guidance.
Onset 3-7 days; peak effect 2-4 weeks; duration 3-4 months.
70-80% experience improvement; repeat injections every 12-16 weeks.
Risks: dysphagia (if sternocleidomastoid over-injected), weakness, antibody formation (5-10%).
Surgical management:
Deep brain stimulation (DBS): bilateral globus pallidus interna (GPi) or thalamic (VIM) stimulation for BoNT-refractory or severe dystonia.
50-70% sustained symptom improvement; potential to reduce medication burden.
Selective denervation surgery: division of spinal accessory nerve (CN XI) branches or cervical dorsal roots for severe, fixed torticollis when BoNT fails.
Stereotactic procedures: thalamotomy or pallidotomy rarely used now given DBS option.
The Procedure (BoNT Injection)
Outpatient, 15-20 minutes.
Key steps:
Patient assessment: determine affected muscles via palpation, observation of deformity.
Muscle localization: EMG, ultrasound, or anatomical landmarks.
27-30G needle; injection of botulinum toxin units (typically 20-200 units per muscle depending on size/hypertrophy).
Multiple injection sites per muscle to ensure diffusion.
Observe 15 minutes; educate on onset/peak timing.
Recovery & Aftercare
BoNT injections: minimal downtime; activity unrestricted immediately.
Avoid massage or vigorous activity 24 hours to minimize spread to unintended muscles.
Peak effect 2-4 weeks; follow-up at 4 weeks to assess response and adjust dose for future sessions.
DBS: 5-7 day hospital stay; programming over 2-3 months; ongoing therapy/PT.
PT continues throughout: stretching, home exercises, postural correction.
Results You Can Expect
BoNT monotherapy: 70-80% experience significant improvement (TWSTRS score reduction ≥25%); 10-15% incomplete or no response.
Symptom relief sustained with repeat injections every 12-16 weeks; some patients develop antibody resistance (5-10%).
BoNT + physical therapy: superior outcomes vs monotherapy.
DBS: 50-70% TWSTRS improvement; additional benefit when combined with BoNT maintenance.
Psychosocial improvement: reduced disability, improved social function, less depression.
Why Choose The Brain and Spine Centre
Led by Dr. Muhammad Aqeel Natt, with expertise in cervical dystonia diagnosis, botulinum toxin injection technique, and surgical intervention (DBS, denervation). EMG and ultrasound-guided injection ensuring accurate muscle targeting and safety. Comprehensive multidisciplinary approach: neurology, neurosurgery, physical therapy, and psychiatry for comorbid mood disorders. Continuity of care with regular reassessment and dose optimization for sustained benefit.
Cost of Torticollis Treatment
BoNT injections: outpatient, repeatable every 3-4 months; cost varies by units/vial.
DBS: significant upfront cost (device, surgery, programming), but durable long-term benefit.
Estimates provided after clinical assessment.
Frequently Asked Questions (FAQs)
Can I know Dr. Muhammad Aqeel Natt’s credentials?
What types of brain tumours do you treat?
Is the surgery safe?
Do I need long-term follow-up after surgery?
Are you having health problems? Contact us today!
Address Business
Contact With Us
Call Us 24/7: 0318 4065914
Working Time
Sunday: 8.30am - 19.30pm