At The Brain and Spine Centre, we specialize in the diagnosis and surgical treatment of neurological and spinal disorders. Dr. Muhammad Aqeel Natt, a leading neurosurgeon in Lahore, provides advanced, safe, and compassionate care for patients.
Carpal Tunnel Syndrome
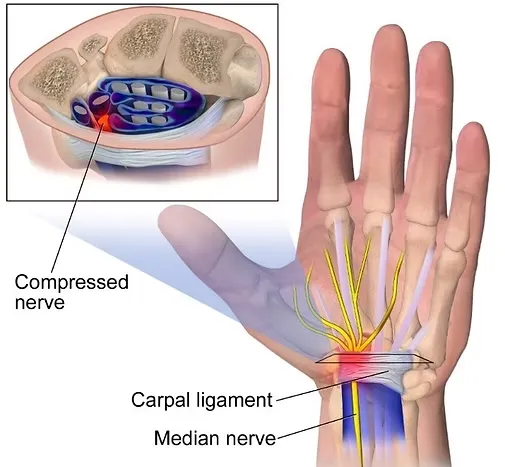
Carpal tunnel syndrome (CTS) is a common nerve compression condition in which the median nerve is squeezed as it passes through the carpal tunnel at the wrist, causing pain, tingling, and numbness in the hand and fingers. At The Brain and Spine Centre, Dr. Muhammad Aqeel Natt offers comprehensive CTS care at Farooq Hospital, West Wood Branch, Lahore, including accurate diagnosis, non‑surgical management, and carpal tunnel release surgery when needed.
Our goal is simple: relieve pressure on the median nerve, resolve pain and numbness, and restore comfortable hand function.
What Is Carpal Tunnel Syndrome?
The carpal tunnel is a narrow passageway in the wrist formed by carpal bones and the transverse carpal ligament; the median nerve and flexor tendons pass through this confined space. Carpal tunnel syndrome occurs when swelling of surrounding tissues or narrowing of the tunnel increases pressure on the median nerve.
Risk factors and causes include:
Repetitive hand and wrist use, including keyboard work, assembly line or vibrating tool use.
Wrist fractures or sprains that deform the tunnel.
Inflammatory conditions (rheumatoid arthritis, gout, tenosynovitis).
Endocrine and metabolic disorders (diabetes, hypothyroidism, pregnancy, obesity).
Cysts or tumours within the tunnel.
Symptoms of Carpal Tunnel Syndrome
Symptoms usually start gradually and may come and go initially.
Common features:
Tingling and numbness in thumb, index, middle, and radial half of ring finger; little finger is typically spared.
“Electric shock” sensations in these fingers, often when holding a phone, steering wheel, or newspaper, or at night; many patients shake out the hand to relieve symptoms.
Nerve pain in wrist/hand that can radiate up the forearm.
Weakness or clumsiness of the hand, difficulty gripping objects, dropping items, or loss of pinch strength from thenar muscle weakness.
In advanced cases, constant numbness and visible wasting of thenar muscles.
Diagnosis
Diagnosis combines history, examination, and electrodiagnostic testing.
Clinical tests: Tinel’s sign (tapping over the median nerve), Phalen’s manoeuvre (wrist flexion), and carpal compression tests reproduce symptoms.
Nerve conduction studies (NCS) and EMG:
NCS measure sensory and motor conduction across the carpal tunnel; slowing or conduction block confirms median neuropathy at the wrist.
Sensory nerve conduction tests are the most sensitive electrodiagnostic measure (≥79.4% sensitivity), while motor tests (e.g., terminal latency index of APB) have high sensitivity (81.3%) and specificity (~98%) when sensory potentials are absent.
Ultrasound may show median nerve enlargement and flattening within the tunnel.
Electrodiagnostic testing also rules out more proximal nerve lesions or generalized neuropathies.
Treatment Options
Management depends on severity and impact on daily life.
Conservative treatment (for mild to moderate CTS):
Activity modification and ergonomic adjustments to reduce repetitive strain.
Night splints holding the wrist in neutral to reduce nocturnal symptoms (weak evidence of benefit, less effective and cost‑effective than surgery but may help short term).
Corticosteroid injections into the carpal tunnel provide good short‑term relief (8–12 weeks) and are more effective than splints, but many patients progress to surgery within a year.
Oral NSAIDs, short courses of oral steroids, and vitamin B6 have limited supportive evidence.
Surgical carpal tunnel release is the definitive treatment for persistent or severe CTS:
Indicated when symptoms significantly interfere with daily activities or sleep and do not settle after at least 8 weeks of splinting and/or steroid injection, or when there is constant numbness, thenar atrophy, or electrodiagnostic evidence of significant axonal loss.
The transverse carpal ligament is cut (open or endoscopic) to enlarge the tunnel and decompress the median nerve.
Surgery has high success rates (75–90%) for long‑term symptom relief, particularly in patients who had good short‑term response to steroid injection.
The Procedure
At The Brain and Spine Centre:
Evaluation: thorough history, physical exam, and, when indicated, electrodiagnostic testing to confirm CTS and grade severity.
Non-surgical phase: trial of activity modification, splinting, and/or steroid injection in early or moderate disease.
Surgical release:
Performed under local or regional anaesthesia, usually as day‑case surgery.
A small open incision or endoscopic portals allow division of the transverse carpal ligament to decompress the nerve.
The procedure typically takes less than 30 minutes and does not usually require overnight stay.
Recovery & Aftercare
Bandage or splint is worn for 1–2 weeks; light finger motion starts immediately to prevent stiffness.
Return to desk work is usually possible within 1–2 weeks; heavier manual work may require 4–6 weeks depending on healing and comfort.
Tingling and night pain often improve quickly; long‑standing numbness and thenar weakness can take months to recover and may not fully resolve if nerve damage is advanced.
Results You Can Expect
With appropriate treatment:
Many mild cases improve or remain manageable with conservative measures alone.
Surgical carpal tunnel release provides excellent long‑term benefit in most patients, with 75–90% achieving significant symptom relief and functional improvement.
Early surgery in severe CTS helps prevent progression to permanent numbness and thenar muscle atrophy.
Why Choose The Brain and Spine Centre
Cost of Carpal Tunnel Syndrome Treatment
Costs depend on whether management is conservative (consultations, splints, injections, NCS/EMG) or surgical (day‑case surgery, follow‑up). A personalised estimate is provided after assessment and discussion of treatment plan.
Frequently Asked Questions (FAQs)
Can I know Dr. Muhammad Aqeel Natt’s credentials?
What types of brain tumours do you treat?
Is the surgery safe?
Do I need long-term follow-up after surgery?
Are you having health problems? Contact us today!
Address Business
Contact With Us
Call Us 24/7: 0318 4065914
Working Time
Sunday: 8.30am - 19.30pm